




Description
Abstract
Bar and clip attachments significantly improve the level of satisfaction of denture-wearing patients by enhancing the retention and stability of the prosthesis. These attachments have been most commonly used for connecting the prosthesis to implants, but they can be effectively used to retain tooth-supported prosthesis as well. The primary functions of bar attachments are splinting the abutments together, even distribution of forces to the abutments and supporting areas, guiding the prosthesis into place, improving the retention, stability, support and comfort of the patient. The primary requirement for the use of bar attachments is the availability of sufficient vertical and buccolingual space for the proper placement of the bar, sleeves, teeth arrangement and sufficient thickness of acrylic denture base to minimise incidence of denture fracture in the area of bar assembly.
Background
The ultimate objective of prosthodontic management is to rehabilitate the patient to as nearly normal function as possible. The basic overdenture concept requires preservation of residual soft and hard tissues. The use of Hader bar1 and clip attachments and adherence to basic principles of complete denture design, drastically improve the level of satisfaction of denture wearing patients by enhancing the retention and stability of the prosthesis thereby increasing the masticatory efficiency.
This case report describes a technique to fabricate the Hader bar and clip attachment retained mandibular complete denture clinically and to explain the advantages that the Hader bar and clip attachment retained mandibular complete denture has over conventional mandibular complete dentures as well as other attachment systems.
Case presentation
A 52-year-old man reported to our dental centre for prosthetic evaluation. The patient had received maxillary and mandibular anterior fixed partial denture and both posterior arches were unrestored. He had difficulty in chewing food and aesthetics due to poor designing of fixed partial denture. He wanted a well-retained prosthesis with better chewing efficiency. After removal of fixed partial denture, clinical and radiographic examination revealed that maxillary and mandibular right and left canines and mandibular right premolar were present, with no periapical pathology. The teeth were periodontally sound with no mobility. Sufficient vertical space was present for the placement of copings, bar and clip, denture base thickness and for the arrangement of teeth. Keeping in mind, the patient’s desire and availability of sufficient vertical space, it was decided to fabricate a maxillary telescopic denture and a mandibular bar and clip retained complete denture.
Treatment
After taking into account all the aspects of the present case, it was decided to fabricate a Tooth and Bar retained and supported mandibular overdenture. On clinical and radiographic evaluation, the remaining abutment teeth (figure 1) were prepared to the desired height, which depends on the availability of the vertical space with tapered round end diamond rotary bur, with subgingival chamfer finish line (figure 2). The impression was made with putty (Aquasil soft putty/regular set, Dentsply, Germany) and light body (Aquasil LV, Dentsply, Germany) polyvinyl siloxane elastomeric impression material by double step putty wash technique and poured in die material to obtain the cast on which a wax pattern of the copings was fabricated with blue inlay wax (Kemdent, UK; figure 3).

Remaining maxillary and mandibular natural teeth.

Widely placed mandibular canines and right first premolar prepared for the construction of bar and copings.

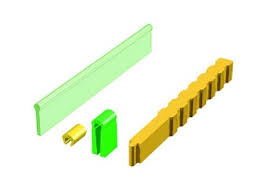
Preci-Horix bar assembly (plastic bar, metal housing, yellow—retention clips, green—fabricating plastic riders and retention clip placement tool).
The distance between the two abutments was measured and marked on the Hader plastic bar (Preci—Horix, Alphadent NV, Belgium). The bar was cut to the desired length and attached to the wax pattern of the copings with blue inlay wax (figure 4), after adjusting the length and height of the bar. The height of the bar should be adjusted according to the availability of the vertical space. The bar should either be in passive contact with ridge or there should be 2–4 mm of space between the bar and underlying mucosa for maintaining proper oral hygiene.2

Plastic bar connected to the inlay wax coping patterns.
The bar and wax pattern of the copings were casted with base metal alloy (Bego Wirocast S, Bego, Germany) and the try in of the finished and polished cast bar assembly was done in the patient’s mouth and the marginal fit of the copings and relationship of the bar with the underlying ridge was evaluated. After evaluation and required adjustments, the casted bar assembly was cemented with glass ionomer cement (Hy-bond Glasionomer CX, Shofu INC, Japan; figure 5).

Casted bar and coping assembly cemented with glass ionomer cement.
After wax up, investing and dewaxing of trial dentures, the Preci-Horix plastic fabricating rider clips was placed on the bar on the master cast at the desired location (figure 6) and then Preci-Horix metal housings were placed over the fabricating rider clips. The under cuts of the retentive bar adjacent to the metal housings were blocked with dental stone and packing was done with heat cure acrylic resin (Lucitone 199 denture base material, Dentsply, Germany), the dentures were processed, finished and polished.

Green fabricating riders for stabilisation of metal housing.
The fabricating plastic riders used for stabilisation of the metal housing during processing of denture were removed with the help of haemostat. The retention sleeves/clips were then placed in the metal housing with the help of a special seating tool supplied in the attachment kit (figures 7 and and8).8). There should be a snap when the clips are pushed into the position. The special shape of the metal housing provides secure retention of the clips while providing leeway space in the labiolingual direction to allow the clips/riders some flex during insertion or removal of the prosthesis. The final prosthesis was delivered to the patient (figure 9). The patient was scheduled for follow-up visits every 3 months and reported no symptomts during 3 years of follow-up.

Retention clips placed in the metal housing with the help of handling tool.

The intaglio surface of the denture with retention clips in processed acrylic denture.

The completed overdenture with much improved retention and stability.
Bar and clip attachments present a reliable and simple solution to denture retention and stability problems by improving the level of satisfaction of patients wearing denture.3 4 Currently, most of these extracoronal attachments are commonly used for retaining and supporting implant prosthesis. Bar and clip attachments can be effectively used to retain and support a complete denture, when a bar is attached to periodontally sound abutments through metal copings. Two abutments, one in each quadrant must be present for bar attachments.
Hader bar can be used as a retainer for tooth as well as implant supported prostheses. The bar is available as prefabricated plastic patterns that are adapted on the master cast and then cast in the alloy of choice. It is the sleeve of the Hader bar system which sets it apart from the other as this is also produced in plastic. The sleeves of most of other bars are made of metal. The plastic sleeve can be easily replaced on chair side when their retention has slackened.
The bar should be positioned directly above the crest of the ridge. This position makes it easy to clean the bar and fabricate the prosthesis above the bar. If the bar is positioned lingual to the crest of the ridge, it will interfere with tongue space and its function and the patient’s speech. If the bar is positioned labial to the crest of the ridge, it will interfere with teeth arrangement and lip support which might affect the aesthetics.
One of the most important requirements for use of any bar attachment is the availability of sufficient vertical and buccolingual space which limits their applications in many instances. Space problems have been stressed for all types of bar retainer, and space is a particularly precious commodity in the lower anterior region. The vertical relationship of the bar to the alveolar ridge is very important. When sufficient vertical space is available, providing 2–4 mm or more space between the bar and mucosa will allow easy passage of saliva and food particles as well as oral hygiene aids. Unfortunately, there is seldom adequate space for this arrangement unless across a cleft palate or an area of gross resorption. So in majority of the patients, the bar needs to be placed in even/passive contact with the mucosa. Any compression of the mucosa by bar will result in hyperplasia of the mucosa. It is impossible to clean underneath the bar, so bar should either be removed or modified to solve the problem.
Hader bar system is more economic and easily available as compare with other bar attachments.5 The vertical height of the plastic Hader bar can be easily adjusted on the master cast before casting, depending on the availability of the vertical space. The retention plastic sleeves can be easily replaced if required. The retention sleeves should be placed in the area of greatest space available.
During the fabrication of bar attachment retained prosthesis, the basic principles of complete denture fabrication must take precedence over mechanical considerations of attachments. The main objective must be to gain support from the maximum possible area to reduce or minimise any displacing loads falling on the denture.
These attachments improve the chewing efficiency and comfort of the patient by reducing the forward sliding of the mandibular denture, maintain the occlusion and minimising the trauma of the underlying supporting tissues.6 7